
Mirocals Status
This page summarises our ‘understanding’ of the current/historical status of the Mirocals trial and the potential Low Dose Interleukin 2 (LD-IL2) treatments arising from it, Proleukin & ILT-101. This page is now sunset but remains for historical context and information.
For all of the historical posts on Mirocals click see our History page.
It is presented as 6 questions and answers below
1) What is the current status of Mirocals trial and the treatment candidate Low Dose Interleukin 2 (LD-IL2)?
Following the Phase II results published in May 2025 no consensus could be achieved on early access and all campaigning stopped. Mirocals, if there is/were any appetite both in the research community and investment community, would require a further scaled trial to progress.
Today, nearly a year later (27th Feb 2026) there has been no activity and we will effectively sunset this page. But it will remain on our website for record.
2) What did we hope Low Dose Interleukin 2 (LD-IL2) might do for MND patients?
The provisional, unconfirmed, results showed a substantial reduced risk of death of between 40% to 70% within the trial period of 21 months.
What could this have meant to us?
If the results were confirmed as positive, it would have not been NOT a cure, however, it could have meant a significant and meaningful slowing of the disease. It would have likely meant months of extra life for many patients and possibly years for some. But there would have been a lot of unknowns. For example, we might not have known how long for or why etc. Only longer use might have shown us, if the drug had been approved
3) How might UK patients have obtained access to the drug if the results were confirmed as positive?
Typically for a new drug, an application to regulators around the globe, eg FDA in the USA, EMA in Europe and the MHRA/NICE in the UK needs to be made. This can typically take 18 months to several years.
Low Dose Interleukin 2 (LD-IL2) would have been no different.
It was envisaged & expected that the pharma ILTOO, who acquired the exclusive rights to the Mirocals data to produce a NEW formulation of LD-IL2 known as ILT-101, would have been applying to the regulators when the data was ready.
But, in a unique aspect of this trial, the active component of LD-IL2, was NOT actually a new drug to the UK healthcare market. It was already approved for some forms of cancer, albeit at a much higher dose. It was/is available as the branded drug Proleukin for these uses. Proleukin is supplied in vials as a powder and is on the NHS price books at an agreed price with the manufacturer.
Importantly, Proleukin was the drug used within the trial and was diluted/compounded to the low dose levels required.
4) How might patients have gained access before a formal approval?
As the regulatory process could have been lengthy, it would have been vitally important to explore all other avenues to seek access for this most exciting and promising treatment this century. Patients did not and so not have the time to wait. How might early access have happened?
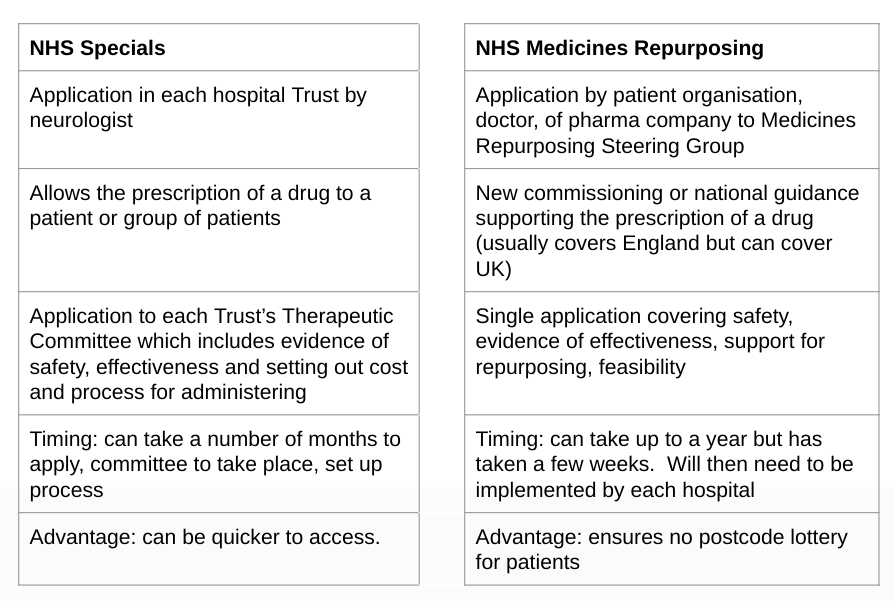
As Proleukin, the drug used in the trial, was an existing drug available on the NHS price books, this opened up two specific access pathways in addition to a new formulation drug regulatory application.
- Off-label prescribing for individual patients (NHS Specials).
- NHS repurposing with national guidance for all eligible patients.
We had encouraged and offered to work with the UK MND charities in preparing for widespread off-label prescription.
We had also asked the charities to work hard for NHS national repurposing guidance on prescription so that no patients missed out. We had awaited news on the progress of the MND Association’s application to NHS repurposing.
We received on (2/11/2023) an acknowledgement by the NHS of the Medicines repurposing application but have been informed that until the data is published in a peer reviewed scientific paper that it will be held in abeyance and placed in monitor status.
IILTOO also announced a Managed Access Program (MAP) which promised to provide some early access to patients to the new formulation, ILT-101. However, this MAP was only available for ex Mirocals trial participants.
5) It was confusing, what’s this about two products, Proleukin and ILT-101?
Proleukin was the form of IL2 used in the trial and for treating some forms of cancer. It had/has, however, stability issues and presents some manageability challenges. If it were to be prescribed after proof of efficacy it would have need recompounding (just as it was within the trial), required chilled delivery in syringes (or be administered in hospitals/care centres) and only be usable for 7 days. But it was a perfectly viable option in patientsunited2endMND’s opinion.
ILT-101 was/is an entirely new form of LD-IL2 under development by ILTOO pharma, that was claimed would be delivered in patient ready syringes that would last up to 36 months.
However, Patientsunited2endmnd and others had concerns about the maturity*, potential availability of, and above all whether the EMA or MHRA would deem that further testing of this new formulation will be required. This latter concern would have been considerably problematic if it were to delay patients receiving LD-IL2 when Proleukin was readily available, even with its manageability issues.
We acknowledged these issues may not have materialised, but, without clarification, we remained very concerned at the time.
*By maturity we were referring to bio-availability, bio-equivalence, stage of development, manufacturing capability and manufacturing quality.
6) What could we do whilst we waited for the eventual disappointing results?
The drug to be put forward for regulatory approval was NOT the drug formulation used in the trial.
We were aware of a number of patients in the UK being prescribed Proleukin privately and managing the administration of the drug as a skin injection 5 days a month.
As patients, it was not for us to recommend or encourage such prescriptions, but we empathised and sympathised with patients facing our disease prognosis.
We therefore urged our scientists and the MND Association to do all they can to expedite the release of the results so patients do not have to take on such risks, and the associated financial hardship, by accessing the drug privately and having to manage its administration without mainstream NHS monitoring and assistance. There was also the health inequality issue, with the vast majority not having the means to take up such an option.
To end this article, we acknowledged that the final results from the trial were not what we had hoped for. So we and the whole MND community have to accept and move on. Move on and keep up the fight.
PatientsUnited2EndMND


{kind=link}